
5-α reductase inhibitors, benign prostatic hyperplasia, and risk of male breast cancer
Robinson D, Garmo H, Holmberg L, Stattin P
Cancer Causes Control. 2015 Jun 25. [Epub ahead of print] PMID: 26109464
Background
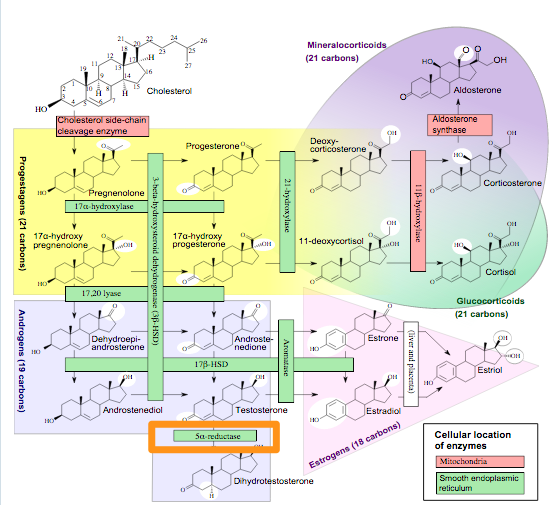
Häggström M, Richfield D (2014). “Diagram of the pathways of human steroidogenesis”. Wikiversity Journal of Medicine 1 (1). DOI:10.15347/wjm/2014.005. ISSN 20018762. – Self-made using bkchem and inkscape
I show this diagram a lot on the blog, because it shows important pathways of hormone synthesis relevant to breast cancer. It is also relevant here, when we are discussing 5-alpha reductase inhibitors that are used to treat prostatic hyperplasia. Five-alpha reductase (orange box) is responsible for converting testosterone into the most active form dihydroxytestosterone. Inhibiting this reaction with a 5-alpha reductase inhibitor can reduce the level of testosterone activity, and so reduce the volume of the prostate.
During the clinical trials of one such inhibitor, finasteride, there were reports of male breast cancer. As it says on the wikipedia page for this drug:
Although overall incidence of male breast cancer in clinical trials for finasteride 5 mg was not increased, there are post-marketing reports of breast cancer in association with its use. Available evidence does not provide clarity as to whether there is a causative relationship between finasteride and these cancers. (Wikipedia, 27 June 2015).
Given that male breast cancer is rare, it is hard to make strong statistical arguments based on the relatively small number of men in the finasteride trials, hence the lack of clarity.
This is where large population studies can be very helpful. Leaders in this area are the Scandinavian countries because they have well organized population and disease registries coupled with a national health system that allows them to follow almost their entire population for their whole lives with detailed medical histories including prescriptions. This enables large retrospective studies of the kind done here, and these contributions are very valuable to understanding risk in human disease.
On the down side, Scandinavia is ethnically not very diverse, and so findings made are likely relevant to people of northern European ancestry, but must be interpreted with care for others.
Findings
What Robinson and colleagues did was look at 124,183 men who had been exposed to the 5-alpha reductase inhibitors and 545,293 controls, and measured the incidence of male breast cancer, and thus calculated the risk.
They concluded that no significant increase in risk of male breast cancer could be attributed to exposure to the 5-alpha reductase inhibitors (5-ARI). Figure 1 (below) summarizes the findings and shows that there was no enhanced risk due to 5-ARI and a borderline enhanced risk due to alpha-blockers.
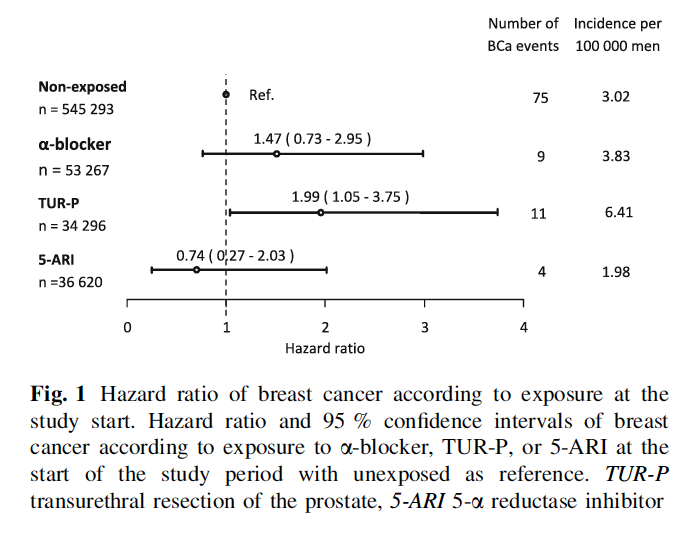
Interestingly, they did find an enhanced risk of male breast cancer in men who had had a transurethral resection of the prostate (TUR-P), an operation for benign prostate hyperplasia (BPH). BPH is hormone-driven growth of the prostate, which may lead to cancer though not inevitably. It is an indicator of a changed “endocrine milieu” as the authors put it.
Comment
This was a Sweden-wide register-based and population-based study, and it is hard to see how a more definitive analysis of the question could be done, realistically. The authors do point to limits – only 99 cases of male breast cancer were captured due to the time-window allowed in the study, and also some other limitations of knowledge regarding the duration of drug taking etc.
Other countries that have similarly comprehensive registries could repeat the study and this would be valuable, but what Robinson and colleagues have done is pretty definitive, within the limits of ethnicity already mentioned. Prospective studies could be contemplated, but they would have to be large and that means expensive (think of all the follow up…). So, I would say, for now this is best evidence we have on this question.
The data are pretty clear on the core question: 5-alpha reductase inhibitors by themselves do not increase risk of male breast cancer. The hypothesis was, I guess, that the increase in testosterone (estimated at 25%) due to the inhibition of 5-alpha reductase could lead to increased levels of estrogens via mass action on the aromatase-catalyzed reaction – but that does not occur – no increase in estrogen is observed and consistent with this no increase in breast cancer risk was seen here. This is good news for men who take 5-alpha reductase inhibitors for their BPH.
The bad news is that men who have surgery for their BPH seem to have an increased risk. There are two possible explanations for this finding. The one closest at hand is that surgery is used in men with the most severe BPH, and so perhaps the most severe change in their endocrine milieu – their hormones, both testosterone and estrogens are higher and they are at increased risk for all hormone-driven cancers. The surgery is a surrogate for a more general risk.
The other possibility, also raised by the authors, is that the ratio of testosterone to estrogen is key for breast cancer risk. This is an interesting idea and the evidence they put forward in support of it can be summarized as follows:
- testosterone-to-estrogen ratio high: no enhanced risk of male breast cancer
- most healthy men
- men with BPH treated with 5-alpha reductase inhibitors
- testosterone-to-estrogen ratio low: enhanced risk of male breast cancer
- men who have had transurethral resection of the prostate (TUR-P)
- men with Klinefelter’s syndrome
- obese men
What I am not sure about is whether it is fair to look at testosterone only in this ratio and not also dihydrotestosterone. This latter variant is the more active form, and it is dramatically lowered when men are treated with the 5-alpha reductase inhibitors (that’s the whole point). This would then move “men with BPH treated with 5-alpha reductase inhibitors” from the upper part of the bullet list to the lower, where they don’t fit because they don’t have enhanced risk of breast cancer. This makes me favor the first explanation more, at least at the current state of knowledge. As usual further study is needed – it is an interesting concept and one that lends itself to experimental analysis both in the lab and in the clinic.
It is also worth noting that the enhanced risk of male breast cancer as a result of the transurethral resection of the prostate (TUR-P) is still pretty low – it adds about 2.5 cases per 100,000 men. As such, the authors end their paper with a sound statement:
[…] we suggest that the concern for breast cancer should not influence the selection of treatment for BPH.
