While there is nothing that forces a strict proportionality between cancer incidence and cancer research funding, there is something to be said for making sure that rare cancers are not left behind. Breast cancer in men is a rare disease, and, from a research funding point of view, it is being left behind.
About 1% of breast cancers occur in men. There is regional variation, with fewer in some countries (e.g. US where it is ~0.7%) and more in others (e.g. Tanzania where it is 6%). Let’s call it 1%.
1% is a small number, for sure, but it is not a negligible number. The American Cancer Society estimates 2,240 breast cancer cases in the US in 2013 for men, and 234,580 for women. Compare the number of breast cancer cases expected in men to the number of men likely to get ALL (3,350), CML (3,420), penile (1,570), bone and joint (1,680), anal (2,630), Hodgkin lymphoma (5,070), small intestine (4,670) and gallbladder (4,470) cancer and it becomes apparent that several recognized cancers have similar numbers.
And yet only about 0.05% of breast cancer funding involves the men’s disease.
Breast cancer overall receives around $1.4bn in research grant funding, according to a recent search of the SciVal Funding database (see Figure; NB not including clinical trials).
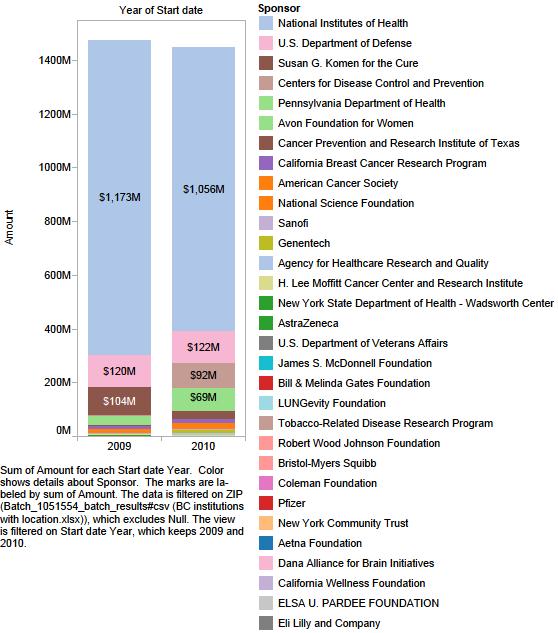
SciVal Funding database search for “breast cancer” led to the identification of around $1.4bn in funding,
In contrast a search of the SciVal Funding database for the term “male breast cancer” revealed only 42 hits. Rather than making a visualization as I did for breast cancer overall and metastatic breast cancer, I thought I would simply look at them, evaluate them for their relevance to the disease and list them here in their entirety.
In summary, it turns out that these 42 hits represent 14 research projects, spanning the entire time in the database, around a decade. Of these there are 4 grants that appear to focus primarily, or at least in large part on male breast cancer – these are numbers 4, 5, 10 and 11 below. The other 10 include male breast cancer amongst many others.
The grant data is incomplete in terms of dollar amounts, particularly with the BCRF grants, and so we can only guess at the total expenditure on male breast cancer research over the past 10 years. Lets add the totals available for male-focused grants, and add half of the support for the ones that include male breast cancer amongst others. If we assume that 4 BCRF grants were $200,000 each which is in the range of many foundation grants, we come to a total of $7.5M over 10 years, or about $750,000 a year.
That spending rate is $334/newly diagnosed man with breast cancer compared to about $6,000/newly diagnosed woman with breast cancer.
So my respectful request to the agencies that fund breast cancer research – and that is primarily the NIH and Susan G. Komen for the Cure – is to devote more funding to projects that include men with breast cancer. 1% of funding would be $14M per year, and represent a 20x increase. Please consider it.
I want to be clear on two points:
First, I am not asking for research on male disease to the exclusion of female disease, but rather more integration of the two. Samples from male breast cancer are becoming more available. But we also need models – cell lines, animals etc The rationale is the same as for the inclusion of metastatic breast cancer, or inflammatory breast cancer, or triple negative etc We need to study the rare variants, even if it is hard to begin with, in order to understand them. Ultimately this knowledge is needed for personalized therapy.
And, second, I recognize that we have learned a lot about the men’s disease from work on the women’s disease and am grateful for this. I recognize this as a biologist and as a patient, whose treatment course has been near-identical to that of my wife, which makes sense as our tumors are also very similar. But, I don’t think we’ve done the research to know what the differences are, and what those might mean for treatment and diagnosis. We can’t assume that the diseases are identical until we’ve done the work.
In short, I am grateful to the work that has been done on women’s breast cancer, and don’t want to take anything away from what is being done there. I wish to stand in solidarity with all breast cancer survivors, with my sisters, and all cancer survivors in advocacy for more research. But I ask that the male disease be remembered.
Here is the list of the grants I found that do include male breast cancer, in chronological order, with most recent first.
1) EORTC Headquarters
This funds infrastructure of the European Organization for Research and Treatment of Cancer. The two entries suggest renewal of the grant or funding of related elements in it and are:
- LACOMBE, DENIS National Institutes of Health, $175,018 01-DEC-2012 – 30-NOV-2013
- SYLVESTER, RICHARD National Institutes of Health, $232,518 01-APR-2011 – 30-NOV-2011
This funding allows US centers to participate in cooperative clinical trials with European collaborators, which is important for rare cancers, such as male breast cancer, where neither region has enough patients to make good progress. This work will include male breast cancer, but is not exclusive to it.
Here is what the applicants wrote (bold by me):
DESCRIPTION (Provided by applicant): The EORTC Headquarters (HQ) is a unique central facility within Europe that offers a comprehensive approach to the management of international, multidisciplinary cancer clinical trials. It provides expertise over a wide range of activities and research areas including data management, statistics, computer science, medical support, regulatory affairs, pharmacovigilance, quality assurance, and quality of life. The goal of this application is to stimulate and facilitate cooperation between the EORTC and US cooperative groups for specific, large scale intergroup trials which will more rapidly bring answers to unmet medical needs. This requires not only coordination of the respective scientific strategies and priorities, but also addresses infrastructure issues to ensure the appropriate conduct of the studies and projects addressed in this application. Besides continuing existing intergroup activities, the EORTC will participate in several new US NCI led randomized phase III studies (brain tumors, pancreatic cancer, cervix cancer) and will take the lead in organizing a prospective intergroup study in male breast cancer. New projects aimed at standardizing procedures to facilitate intergroup cooperation will be undertaken together with our US partners. This includes the development of a platform to facilitate the use of imaging in multicenter intergroup trials, the harmonization of quality assurance programs in radiotherapy (QART), and the further development of RECIST. Additional joint initiatives will also be explored in areas such as clinical trials in the elderly and in rare diseases along with the development of joint trials in lung cancer and collaboration to harmonize biobanking activities for translational research. Through these joint initiatives, new intergroup clinical trials will be undertaken which would be difficult for either organization to carry out by themselves and which should have a major impact on day to day clinical practice on a worldwide basis.
2) Technology to improve the assessment of tissue-associated protein biomarkers
- BALTIMORE VA MEDICAL CENTER MASON, JEFFREY THOMAS U.S. Department of Veterans Affairs, $ Not Available, 01-OCT-2012 – 30-SEP-2013
This grant is about technology development for better detection of breast cancer, and is not specific to men, as can be seen from the abstract, where there is one sentence towards the end, which I bolded. Of course, currently most veterans are still men. Here is the abstract:
DESCRIPTION (provided by applicant): The identification of patients at high risk of recurrence is one of the most important assessments in the clinical management of breast cancer. Sentinel lymph node status is the current gold standard for clinical discrimination between good and poor prognosis and for deciding if patients receive adjuvant chemotherapy following surgery. However, ~30% of women with node-negative status experience recurrence within 10 years of initial treatment, while ~25% of women with node-positive status do not. Accordingly, there is a need for additional prognostic methods to assess recurrence and survival in breast cancer patients. Urokinase-type plasminogen activator (uPA) and plasminogen activator inhibitor type-1 (PAI-1) have been validated at the highest level of evidence (LOE-1) as clinical biomarkers of prognosis in breast cancer. The American Society of Clinical Oncology recommends using uPA and PAI-1 levels in breast tumors for the routine assessment of prognosis in patients with newly diagnosed breast cancer and for deciding whether node-negative breast cancer patients can forgo adjuvant chemotherapy. The sole validated method for quantifying uPA and PAI-1 levels in breast tumor tissue is a colorimetric ELISA assay requiring a minimum of 300 mg of tumor tissue. Generally, only open (excisional) biopsy will yield 300 mg of tissue, while the more common vacuum-assisted core needle biopsies yield d 110 mg of tumor tissue. The 300 mg requirement also places a restrictive lower limit on the size of tumors that can be evaluated. Accordingly, the availability of a reliable method to accurately quantify uPA and PAI-1 levels in d100 mg of biopsy tissue would have a profound impact on the clinical management of breast cancer. The objective of the studies outlined in this proposal is to develop technologies to rapidly and accurately quantify levels of uPA and PAI- 1 in small tissue specimens (10-100 mg) obtained by fine needle core biopsies of breast tumors. Our central hypothesis is that the combined use of an innovative pressure cycling technology to solubilize tissue proteins and a novel and highly sensitive immunoassay format, called immunoliposome-polymerase chain reaction (ILPCR), developed in our laboratory will achieve the level of quantification for uPA and PAI-1 stated in our objective. The rationale for these studies is that their successful completion will provide clinicians with more reliable means to determine those node-negative patients most likely to benefit from adjuvant chemotherapy following surgery for beast cancer. Accordingly, our project proposes the following three specific aims. Aim 1 is to develop and optimize a method to rapidly and quantitatively extract soluble uPA and PAI-1 from breast tumor tissue using rapid pressure-cycling technology. Aim 2 is to develop and optimize ILPCR assays that can accurately quantify uPA and PAI-1 from 10-100 mg of breast tumor tissue with an assay sensitivity and specificity of e95%. Aim 3 is to validate the rapid pressure-cycling extraction method and ILPCR assays for uPA and PAI-1 against the “gold standard” ELISA assay by using tissue obtained from the same breast tumor for both assays. These studies are innovative because they will overcome a critical barrier to the use of uPA and PAI-1 for the prognostic evaluation of breast tumors. This research will also improve clinical practice because it will provide clinicians with more reliable means to determine those node-negative patients most likely to benefit from adjuvant chemotherapy, particularly those patients with hormone receptor-negative and node-negative grade 2 tumors who are borderline candidates for chemotherapy. Finally, this research is relevant to Veterans and the VA health care system because it will improve the survival and quality of life of breast cancer patients. It will also facilitate the detection and prognostic assessment of breast tumors at earlier stages where clinical options are greatest and where treatment outcomes are most likely to be favorable. PUBLIC HEALTH RELEVANCE: Breast cancer is the second leading cause of cancer death among women. With the average age of female Veterans approaching 48, the incidence of breast cancer in the VA population will start to rise. This escalation will continue because women are now the fastest growing subgroup of U.S. Veterans. Although the incidence of male breast cancer is low, environmental factors experienced in military deployment may lead to an increased risk of breast cancer in both men and women. The assays to be developed in this project will provide clinicians with more reliable means to determine those node-negative patients most likely to benefit from adjuvant chemotherapy following surgery for breast cancer. This will result in decreased patient morbidity and mortality providing improved quality of life for Veteran breast cancer patients. The associated reduction in cancer recurrence will also lead to a decrease in overall patient burden and health care costs for the VA medical system.
3) Chemoprevention of Prostate Cancer
- NEW ENGLAND RESEARCH INSTITUTES, INC. National Institutes of Health, $258,800 01-SEP-2011 – 31-AUG-2012 United States
As the title suggests, this one is about prostate cancer, and investigates a drug used there for chemoprevention, finasteride, which has been implicated in increasing risk for male breast cancer. Not really a male breast cancer grant.
4) Clinicopathological characterisation of Male Breast Cancer
- Peter MacCallum Cancer Centre Deb, Siddhartha National Health and Medical Research Council, $Not Available 01-JAN-2011 Australia
This appears to be the real deal, from our colleagues at the PeterMac in Melbourne! No details in the grant database though. I found a newsletter that has the following description of the work in it:
[NHMRC Postgraduate Scholars] Two clinicians who constitute the link from ‘bench to bedside’ are Anatomical Pathologist, Dr Siddhartha (Sid) Deb and Victoria (Tori) Mar, who were both awarded prestigious NHMRC scholarships. Specialising in breast cancers in men, Sid will shift his research focus, analysing data that address clinical questions that arise from his everyday work. ‘At Peter Mac I have a great opportunity to perform translational research within a cancer centre that houses research-focused clinicians alongside excellent scientific laboratories’. Sid’s research proposes to be the largest study to molecularly characterise male breast cancer, establishing a cohort for extensive clinicopathological investigation and allow valuable assessment of genotypic-phenotypic patterns to hopefully contribute to the development of novel treatment strategies for breast cancers. ‘This grant will allow me to utilise my clinical training in a research setting, something I may not be able to do elsewhere.’
We then have a series of 4 grants (number 5-8 below) from the Breast Cancer Research Foundation (BCRF) for the years 2010-12, which together make up 14 hits in the database, because multiple investigators are involved in each. They are:
5) BCRF: Breast International Group (BIG) and The North American Breast Cancer Groups (NABCG)
This is a collaboration between three countries – Canada, US and Portugal – to collect male breast cancer cases and samples. It is the real deal, and you can read more about it on the BCRF website. One of the PIs is Dr. Sharon Giordano, my oncologist, at MD Anderson (yay!). It is about:
Due to the low incidence of male breast cancer, international cooperation is necessary to undertake relevant projects with potential clinical impact. With the support of BCRF, the Male Breast Cancer International Registration and Biologic Characterization Program has been launched as a joint effort between the Breast International Group (BIG) and the North American Breast Cancer Groups (NABCG) and coordinated by the European Organization for the Research and Treatment of Cancer (EORTC). In the first part of this program, clinical data and tumor samples from about 1,500 male breast cancer cases are being collected. Accrual to these studies is happening rapidly, and over 400 patients have registered. This is the largest study on male breast cancer to date. The pathology analysis of these tumor samples in the central labs will lead to a better understanding of the biological characteristics of this disease and to the identification of important potential prognostic (indicative of the good or bad outcome of the disease) and predictive (indicative of probability of response to certain therapies) markers. The second part of this program, a prospective registry, is about to be launched.
6) BCRF: Various projects on behalf of SWOG
BCRF has funded various studies related to SWOG clinical trials (SWOG is a cooperative group of institutions that work together on clinical trials), including a biological characterization of male breast cancer. It is unclear how involved this male trial is in current investigations from the write up on the BCRF website.
7) BCRF: Highly Agressive Breast Cancers
Work from Sofia D. Merajver, MD, PhD on a variety of rare cancers across the globe is also supported by BCRF. Again this includes male breast cancer and in part the write up on the website says:
Furthermore, Dr. Merajver’s team has also completed a landmark study on male breast cancer in Uganda and Egypt and will continue with their efforts in characterizing the molecular genetics of aggressive breast cancers in Africa.
However, this doesn’t sound as if male breast cancer is the major focus, but is included alongside other cancers.
8) BCRF: On behalf of The North American Breast Cancer Group and the Breast International Group
A grant in support of coordinating work across these two groups in several areas, this one includes male breast cancers amongst others, as per the description on the BCRF website:
The main structure of this effort is divided into eight research areas: Immunology, Metastatic Breast Cancer, Survivorship Working Committee, Male Breast Cancer, Endocrinology, Triple-negative Cancer, HER2, and Biomarker. This collaboration facilitates the pace of translation of new agents and technologies into clinical use and avoids unnecessary duplication of effort.
The grants appears to support the coordination more than the work itself.
There was one other hit in the database for BCRF on a grant from Dr. Monica Morrow of Memorial Sloan-Kettering Cancer Center, but the only part of the abstract that made it was:
In contrast to their female counterparts, men rarely develop breast cancer. In the US, less than 1% of all breast cancers are diagnosed in men. Doctors have a limited understanding of how to approach such an uncommon disease. Most decisions …
However the link to the BCFR site is broken, and when you search the site for ‘Morrow’ you only find a pdf of a newsletter that lists her, but does not describe her work. Pubmed shows papers by Dr. Morrow, but none of the specifically adress the male disease. Perhaps the research never completed.
9) Validating CYP2D6 genotype-guided tamoxifen therapy for a multiracial U.S. population
- University of North Carolina at Chapel Hill, Irvin, William, Susan G. Komen for the Cure, $449,714 01-JAN-2009 United States
This is a grant to develop a biomarker to guide use of Tamoxifen, and so perhaps includes men, but is not focused on it. Here is a part of the lengthy abstract which can be read on page 96 of this PDF:
Tamoxifen is one of the most commonly used drugs in the treatment of breast cancer. It is the only approved adjuvant (in addition to surgery) drug for endocrine therapy in pre-menopausal women, and it is also used to treat hormone receptor positive (HR+) metastatic breast cancer; HR + male breast cancer; post-menopausal, HR + breast cancer; treatment of the precancerous condition ductal carcinoma in situ; and to prevent invasive breast cancer in women who are of high risk.
10) Prostate Derived Ets Factor, An Immunogenic Breast Cancer Antigen
- ROSWELL PARK CANCER INSTITUTE, BUFFALO, SOOD, ASHWANI K., U.S. Department of Defense, $126,539 01-JAN-2004 – 31-DEC-2004 United States
This grant supported an interesting study to see if self-immunization across genders could be used for clinical benefit. The abstract said:
Goals and Objectives: The vaccine/immunotherapy approach to prevention and treatment of breast cancer is highly attractive since (1) side effects are expected to be low; (2) women likely to benefit may be predicted by analyzing the quality and quantity of their immune responses to specific antigens; and (3) long-term antitumor immunity may be established and boosted periodically to maintain surveillance against any arising disease. We recently made an unexpected observation that vaccination with a self-antigen (Pse) significantly delays breast tumor development in mice. These results are contrary to published reports showing that self-antigens induce poor immune responses with little anti-tumor effects. Our concept is that Pse works as a foreign antigen in female mice, and this allows induction of a strong immune response with significant antitumor effects. The objectives of this study are to test this concept.
Relevance: Validation of the concept proposed here will provide rationale to test whether vaccination with human counterpart of Pse self-antigen also will induce strong antitumor immune responses in female breast cancer patients. A novel avenue of research arising from the latter study will be: (1) to identify the specific immune cells that show anti-tumor effects and (2) to determine if transferring the specific genes from anti-tumor immune cells of female breast cancer patients to male breast cancer patients will enhance the immunologic competence of male patients against their tumors. Overall, this research will enhance the application of vaccine/immunotherapy approach against breast cancer.
Because this work directly addresses the needs of male breast cancer patients alongside women, I consider it to belong to the group of grants focused on male disease.
I cannot find a specific paper related to this work in PubMed, which would be expected over 8 years after funding completed, but the PI is active in this area, and has a recent review in the general area of immunotherapy for breast cancer.
11) Mammary Gland as a Sensitive End Point to Effects of Endocrine Disruptors
- ENVIRONMENTAL HEALTH SCIENCES, FENTON, SUZANNE, National Institutes of Health, $2,865,961 United States
- ENVIRONMENTAL HEALTH SCIENCES FENTON, SUZANNE, National Institutes of Health, $1,574,798 United States
- ENVIRONMENTAL HEALTH SCIENCES FENTON, SUZANNE, National Institutes of Health, $2,040,573 United States
This multiply renewed grant supports work that looks at environmental triggers for breast cancer and includes men, as is stated in the abstract:
[…] We have made major progress on our work involving investigation of dry cleaning solvents and their developmental exposure effects on the mammary gland, specifically in males. These compounds are theorized to have a role in male breast cancer diagnoses in men who were born or grew up at the Camp Lejeune military base in NC, USA. We have finished dosimetry studies in the pregnant and lactating rat and her offspring in conjunction with our CDC collaborators. We have evaluated mammary gland development and will soon prepare a manuscript on the effects of these compounds on male and female mamamry glands. We have also begun studies to look at susceptibility to mammary gland hyperplasia in female mice exposed to bisphenol A (BPA), BPAF and BPAS (fluorinated and sulfonated forms)in early life. […]
This grant includes men alongside women, and focuses on the Camp Lejeune cluster, and so I believe is an important contribution to understanding the male disease.
12) Studies of Atomic Bomb Survivors
- CANCER EPIDEMIOLOGY AND GENETICS, MABUCHI, KIYOHIKO, National Institutes of Health, $860,011 United States
- CANCER EPIDEMIOLOGY AND GENETICS, MABUCHI, KIYOHIKO National Institutes of Health, $347,101 United States
- CANCER EPIDEMIOLOGY AND GENETICS BERRINGTON, AMY National Institutes of Health, $71,026 United States
- CANCER EPIDEMIOLOGY AND GENETICS, BERRINGTON, AMY National Institutes of Health, $651,468 United States
- Unspecified, LAND, CHARLES, National Institutes of Health, $Not Available, United States
This multiply renewed grant includes epidemiological analysis of a broad spectrum of cancers, including rare tumors like male breast cancer. As the abstract states in part:
The long -term temporal pattern of leukemia risk is currently investigated. Among several new findings are the radiation-related excess risk of male breast cancer.
13) Studies of Rare Cancers
- CANCER EPIDEMIOLOGY AND GENETICS, BRINTON, LOUISE, National Institutes of Health, $1,205,252, United States
- CANCER EPIDEMIOLOGY AND GENETICS, BRINTON, LOUISE, National Institutes of Health, $1,280,000, United States
- CANCER EPIDEMIOLOGY AND GENETICS BRINTON, LOUISE National Institutes of Health 1,537,322 United States
- CANCER EPIDEMIOLOGY AND GENETICS BRINTON, LOUISE National Institutes of Health 934,284 United States
Two entries suggests this grant was renewed. This grant supports epidemiological assessment of rare cancers in general, and include male breast cancer, as part of the abstract describes:
We have recently extended our interests in the etiology of breast cancer to also include a focus on rarely occurring male breast cancers. In an analysis within the large NIH-AARP cohort study, we identified that a family history of breast cancer in a female relative, obesity, physical inactivity and a history of bone fractures related to increased risk. An investigation within the U.S. Veterans Affairs computerized medical care system database found increased risksof male breast cancer associated with hospitalizations for Klinefelter syndrome, obesity, diabetes, gynecomastia, orchitis/epididymitis and cholelithiasis (latter only among African Americans). We are currently following up these findings in a pooled analysis in which are including data from the majority of case-control and cohort investigations. Cohort investigations will be particularly valuable towards assessing relationships with genetic markers and endogenous hormones. We are also hoping to obtain breast cancer tissue samples from some of the studies.
14) Descriptive Studies and Record Linkage
- CANCER EPIDEMIOLOGY AND GENETICS, ANDERSON, WILLIAM, National Institutes of Health, $1,793,379 United States
- CANCER EPIDEMIOLOGY AND GENETICS, ANDERSON, WILLIAM, National Institutes of Health, $691,140 United States
- Unspecified, ANDERSON, WILLIAM, National Institutes of Health, $1,551,349 United States
- Unspecified, DEVESA, SUSAN S., National Institutes of Health, $Not Available, United States
This is another grant that looks at cancer very broadly, and includes male breast cancer in its analyses, as described in the abstract:
The Black and White ethnic crossover was a robust feature in the SEER database. Amidst recent declines for female breast cancer, age-adjusted incidence rates may be increasing for male breast cancer in the United States (US) and elsewhere. However, age-adjusted temporal trends reflect an age-specific weighted average, which may be confounded with age-related biological and/or temporal effects (period and/or cohort). We, therefore, supplemented the descriptive epidemiology of male and female breast cancer with age-period-cohort (APC) models, simultaneously adjusted for age, calendar-period, and birth-cohort effects. Results showed that male and female breast cancers demonstrated similar secular trends but different age-related biology; i.e., relatively more late-onset, low grade and ER positive tumors among men than women. A large-scale population-based comparison of male and female breast cancers demonstrated three intriguing results. Age-specific incidence patterns showed that the biology of male breast cancer resembled the late-onset type of female breast cancer. Similar breast cancer incidence trends among men and women suggested that there are common breast cancer risk factors that affect both sexes, especially estrogen receptor positive breast cancer. Finally, breast cancer mortality and survival rates have improved significantly over time for male breast cancer, but progress has lagged behind for men compared to women

Wonderful thank you Oliver we are totally behind you! http://www.CHECKTHEM.org amd http://www.BREASTSELFEXAMS.org
Save a Life today it maybe YOUR own Share with all you love!
You’ve made a really compelling argument here. I agree that we need more information about possible sex differences. As a layperson, it fascinates me that there’s a higher proportîon of male breast cancers that are ER/PR positive than for women. And the high variation in incidence rates across countries is also interesting. As you know, this variability is well documented in female breast cancer with the U.S. having a 12 percent incidence and many other countries having much lower lifetime incidence despite the current estimate that only 5 percent of female breast cancer have a genetic etiology. And on top of that, some of the countries with low incidence have terrible pollution problems! This is one of the reasons I have concentrated on shared diet and lifestyle factors across the low incidence countries. Since they are healthy things to eat and do anyway, it fits perfectly into my tainted test tube approach.
Elizabeth – yes, there must be some interesting biology out there. Coincidentally I spoke with one of the top genome scientists today who is sequencing my cancer and he said that preliminary analysis showed it was pretty quiet on the mutation front. More on that when I know more but he said the lack of much data on other men made it hard for him to compare it to anything meaningful.
Yes, let us know what he has to say. I’m sorry he doesn’t have a good frame of reference but happy that you have access to people like him.
Reblogged this on My Eyes Are Up Here and commented:
Oliver makes a compelling argument for increased funding for male breast cancer. His breast cancer is treated using the same protocol as female breast cancer because there is so little research guiding best practices for men. And last I noticed, there were some biological differences between males and females of the human species. Finally, Oliver makes a strong argument without oversimplifying, being sarcastic, or being disrespectful. His data and reasoning are compelling enough to elicit a desired emotional response like compassion and a call to action.
Thanks Oliver! So glad you are in our corner! Hope that your efforts bare fruit in the form of increased funding for the cause. Very good presentation.
As always an informative dissection of the current data on male breast cancer combined with practical information for fellow patients. Your voice is important for all male breast cancer patients as is your courage to share your story.