In another month or so, I am joining an immunotherapy clinical trial that is aimed at suppressing recurrence, by training the immune system to pay attention to cancer cells more effectively.
It is a trial designed by Dr. Beth Mittendorf, who recently spoke about her work in an interview .
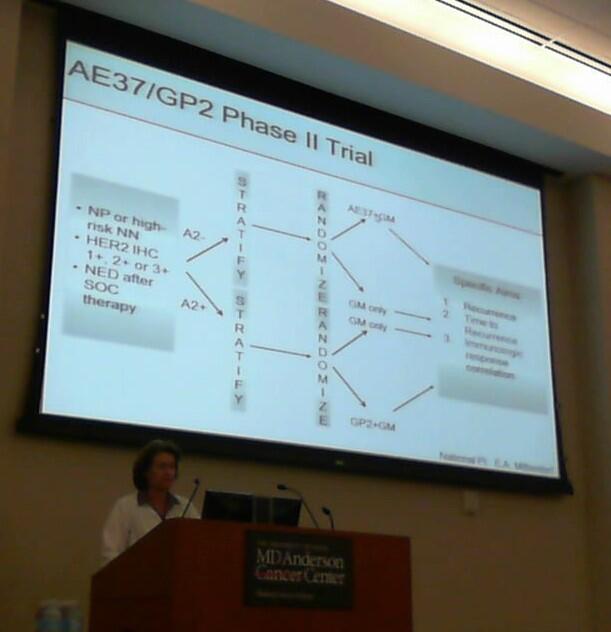
The trial I am joining is “Prospective Randomized, Single-Blinded, Multi-Center Phase II Trial of the HER2/neu Peptide GP2 + GM-CSF Vaccine versus GM-CSF Alone in HLA-A2+ OR the Modified HER2/neu Peptide AE37 + GM-CSF Vaccine versus GM-CSF Alone in HLA-A2- Node Positive and High Risk Node-Negative Breast Cancer Patients to Prevent Recurrence”.
That’s quite a mouthful, and is meant to tell you all about the trial.
Let’s break it down.
The overall goal of the trial is to help the immune system with surveillance of breast cancer cells that might have survived all the other treatments. It does so by drawing attention to the Her2 protein. Many breast cancer cells, at least of luminal subtypes, express more Her2 than normal cells, even if they don’t express the ultra-high levels that earn them the Her2+ designation and the option to be treated with Herceptin. So by knocking down Her2 expressing cells the immune system can keep any remaining cancer cells in check.
The trial focuses the attention of the immune system on Her2 with either of the two peptides being used, which are called GP2 or AE37. These are small bits of the Her2 protein, and are known to be good epitopes, which means a structure that is good at attracting the attention of the immune system. Imagine that you are trying to identify a car that is passing fast at night. Not all parts of the car may be clearly visible. The headlight is likely to make a stronger impression on you than, say, the door. You could teach someone who had never seen the car to recognize it by showing them only the headlight if it was a sufficiently distinctive one (ie a good epitope).
Why do we have two peptides, doing the same thing? Well, this is for simply practical reasons. It turns out that in some people GP2 works well, and in others AE37.
The reason is the platform that the immune system uses to recognize the peptide comes in different versions. Here the trial distinguishes between people are HLA-A2 positive or negative. HLA are part of the immune system, and you can think of them similar to blood type. HLAs are sort of like the platform the immune system uses to recognize abnormal or foreign bodies, and depending on which platform you happen to have, the trial uses either the GP2 or the AE37 peptide. You can think of this as playing a video game on Xbox or Playstation – its the same game, but if you have the Xbox disk (here peptide) you aren’t going to be able to play it on a Playstation (HLA). The peptide and HLA have to be compatible. Patients are first typed for HLA-A2 type and then assigned to the appropriate group.
So what is the GM-CSF? GM-CSF is a cytokine, a member of a large class of molecules that immune cells use to communicate. When, in the normal course of an immune response to say a bacterial infection, one immune cell wants another one to pay attention to the bacteria, it can use such cytokines to attract their attention, and actually allow them to proliferate. In this trial it is a critical tool to activate the immune reaction to the Her2 peptides. Without it, the immune system, which is bombarded by many signals every day, could miss that this Her2 thing is something it should really pay attention to.
The trial requires several rounds of immunization with the peptide-cytokine cocktail. Why? This is because we know that repeated exposure to an antigen is another good way to get the immune system to pay attention. There is a part of the immune system that keeps a memory, that makes you immune. This is why getting vaccinations as a kid can protect you for many years. And the immune system benefits from repetition, just like a kid learning their vocabulary.
By the way, when I say above “we know” what I mean is that many many years of research by many immunologists has shown these things, and has established the principles and understanding that underlies this entire field. It takes a lot of basic research to get the field to a point where successful clinical interventions become possible.
Preliminary results from trials of this kind are quite promising. A recent publication showed that 2-year disease free survival was increased by around 10% for lymph-node positive patients with low and intermediate levels of Her2. Futhermore, none with booster innoculations have recurred.
Sign me up!

Thanks for volunteering and helping others!!
Those are encouraging preliminary data. Good luck!
Hi, thank you for excellent posts. What a shame I didn’t discover it earlier; I would love to read it while in treatment. I was diagnosed last year with very rare and very aggressive CCC in breast, tripple negative. Although I finished my very harsh treatment at Christmas, I wasn’t able to write about it until recently actually. Because I am from Europe and things are a bit different here, I am trying to raise some awareness that even young people can get cancer too. I was struggling to find information about my diagnosis ( as did the doctors too) and was desperately searching for info even contacting all big names in the play in the US like MD Anderson, Sloan Kettering etc. Now, I am sharing my experience in the Cancership blog ( http://www.cancership.com) and starting to work with oncological patients as a psychologist…
I wish you and your wife all the best. Stay strong.
Petra
I enjoyed reaading your post