
Prediagnostic Sex Steroid Hormones in Relation to Male Breast Cancer Risk
Brinton LA, Key TJ, Kolonel LN, Michels KB, Sesso HD, Ursin G, Van Den Eeden SK, Wood SN, Falk RT, Parisi D, Guillemette C, Caron P, Turcotte V, Habel LA, Isaacs CJ, Riboli E, Weiderpass E, Cook MB
J Clin Oncol. 2015 May 11. pii: JCO.2014.59.1602. [Epub ahead of print]
Background
Most breast cancers are hormone driven. Most male breast cancers are estrogen and progesterone receptor positive and respond to hormone therapy. But are hormones involved in the origin of the cancer? For women this is well established. For men, no one had looked, until now.
On a personal note, one of my colleagues – a breast cancer medical oncologist, though not my treating oncologist – told me that the most effective part of my therapy was likely to be Tamoxifen. And I did wonder why my estrogen levels were not measured during my pre-treatment workup, or for that matter now that I am on Tamoxifen – believing they are waaay low is not hard though ;-).
Here then is the first direct analysis of the question of whether elevated hormones are associated with male breast cancer. It is a very logical study that fills an important gap in knowledge. It is not surprising that it was published in the prestigious Journal of Clinical Oncology, a flagship journal of the American Society of Clinical Oncology!
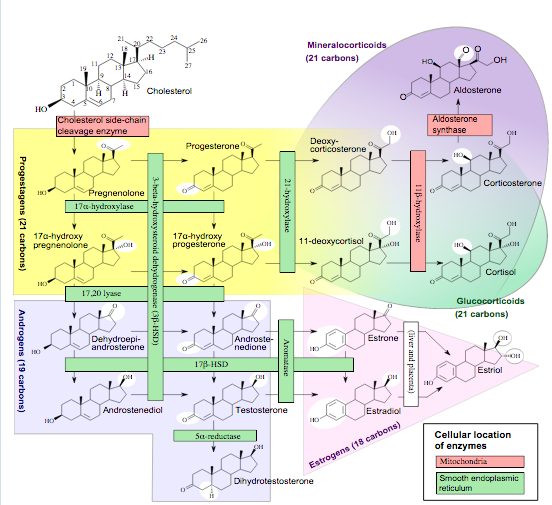
Häggström M, Richfield D (2014). “Diagram of the pathways of human steroidogenesis”. Wikiversity Journal of Medicine 1 (1). DOI:10.15347/wjm/2014.005. ISSN 20018762. – Self-made using bkchem and inkscape
This image shows the metabolic pathways of estrogens, with many of the hormones that were analyzed in this study.
Findings
Underlying this study is a pooling project, in which 7 groups pooled male breast cancer cases and matched controls for the analysis. Groups were form the UK, Norway, Europe and 4 from the USA. Nevertheless, only 101 breast cancer cases (and 217 controls) were included – a good number of such a rare tumor, but small when compared to similar studies on the women’s cancer. Key of course was that a blood sample suitable for hormone analysis was available from before the diagnosis was made, and this probably restricted the samples that could be included.
The authors analyzed 9 hormones and metabolites of hormones using standard tests, and studied the statistical correlation to risk of getting breast cancer. They also studied the interrelationship of different hormone levels.
The key finding is that elevated estradiol is associated with elevated risk of breast cancer. Estradiol or E2 is both the most prevalent and most potent of the estrogens. In more detail, the authors found that the quartile with the highest E2 had a 2.5-fold higher risk of having male breast cancer when compared to the lowest quartile. Imagine 100 people lined up in the order of their estradiol levels. The 25 at the “higher” end have a 2.5 fold greater chance than the 25 at the bottom of getting this disease. This is significant, and not dissimilar from hormone-related risks found for women with breast cancer. Furthermore, when the authors divided the cases into those diagnosed below the median age (67) and above it, they found that higher estradiol-associated risk peaked around 3-fold.
Comment
So what does this mean?
Increased risk is always a concern. However, it should be noted that a 2- or 3-fold risk of something that is low risk is not itself a reason to rush to your doctor and get an estradiol test. If your chance of getting this disease is, say, 1 in a 100,000 with low estradiol, it would now be 2 or 3 in 100,000. In other words, still low. Still, it might mean that one can use hormone tests for screening or surveillance of people at elevated risk. If a very low cost test, perhaps incorporated into a whole battery of other tests (think future technology) is developed, keeping an eye on estradiol might make sense for the general population, even.
Perhaps more importantly, this finding sheds light on the fact that increased hormone levels could well have a causative or contributory role in the origin of male breast cancer. This is again not a huge surprise – we know that most male breast cancer is ER/PR positive and responds very well to hormone suppression therapy. This is in itself biologically interesting – it may lead to definitive understanding of the similarities (and hence differences) between hormone-driven breast cancer in men and women.
Interesting in this context is also the finding that breast cancers in younger men was more affected by increased estradiol, and this is reminiscent, as the authors discuss, of the differences in risk factors and biological drivers of breast cancer in different age groups of women.
On a personal note, again, I was very excited to see this paper and applaud the authors for investigating this important issue.
