
Metastatic Male Breast Cancer: A Retrospective Cohort Analysis
Robert Foerster, Lars Schroeder, Frank Foerster, Volker Wulff, Birgit Schubotz, Dieter Baaske, Christian Rudlowski
Breast Care 2014; 9:267-271
Background
This paper addresses an understudied area – how men with metastatic breast cancer fare. It is a retrospective analysis, and so contributes to the baseline knowledge that will help us develop new approaches in the future. It meets a need as there is very little data on men with breast cancer, and almost all treatment decisions for men are made on the basis of data from studies of women – there are no treatment guidelines for men with metastatic breast cancer. This is an important contribution to the field for these reasons alone.
Findings
Researchers in Germany (including at the NCT which together with the DKFZ, the German Cancer Center is an important partner in MD Anderson’s Global Academic Program Sister Institution network) gathered 160 men with breast cancer, of whom 41 had metastatic disease. Of these 41 about 40% already had mets at the time they were diagnosed, while the remaining 60% showed mets upon recurrence.
Mets went preferentially to the bone and lung, with liver and brain less common.
Median survival from occurrence of mets was 32 months – this means that of the 41 men with metastatic disease, half died in under 32 months and the other half after that. (By comparison, median overall survival from first diagnosis, including all the men in the study, so also those with no mets, was 68 months.)
Men who received systemic therapy (i.e. therapy that reached the whole body, which typically means drugs such as chemotherapeutics or anti-hormone therapy; as opposed to surgery and radiation which are local or regional) did better. This is shown in the figure below, and although no medians are stated, it looks like these therapies add on average 10-20 months of survival.
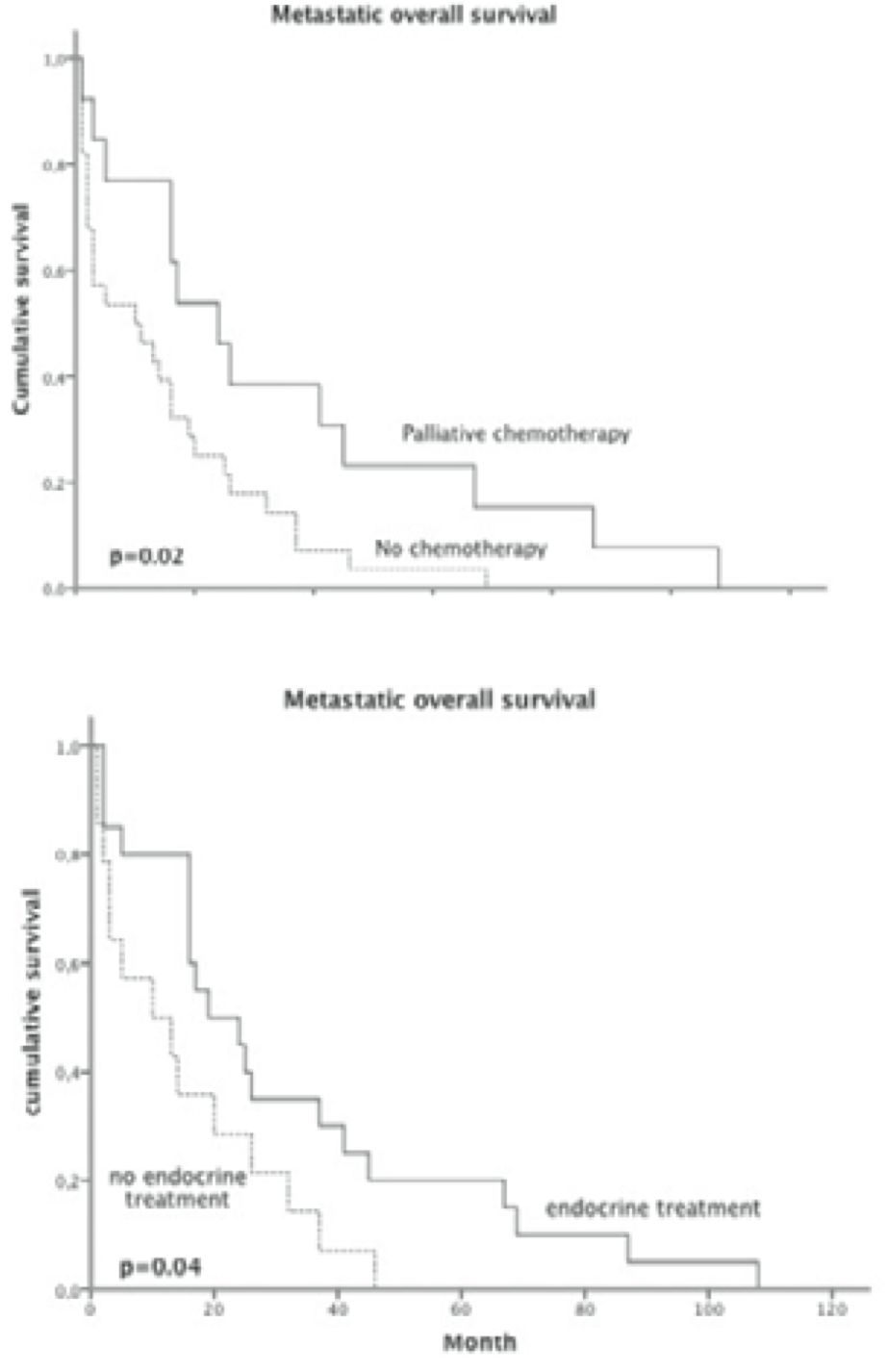
Survival of men with metastatic breast cancer is improved by systemic therapies.
Importantly the authors discuss these findings in the context of data on women, and point to reasons why their data may look different:
Our patient group is characterized by a median [metastatic overall survival] […] well below values published by Giordano et al. [9] for women with metastatic disease diagnosed in between 1995 and 2000 […]. However, when comparing our results to those of women initially diagnosed between 1990 and 1994, similar values can be found […]. This could be explained basically by the underpowered palliative treatment of [metastatic male breast cancer] documented in our cohort.
In other words, the male cohort studied here, which was collected between 1995 and 2011, did not receive the latest in palliative therapy, which may have increased mortality. Again, this points to the importance of systemic therapies at all stages.
Overall the authors conclude:
Therefore, it seems reasonable that treatment of MMBC should be based on the guidelines for female breast cancer.
Comment
It’s excellent that a study on metastasis in male breast cancer was done – kudos to the authors and my thanks.
It is reassuring that the evidence supports current practice – to model therapy for men on what is used for women. It is also reassuring that systemic therapies are effective – both hormone therapy and chemotherapy. In other words, we have approaches that make a difference. Of course, they have their price and they are not curative.
In the discussion the authors touch on endocrine therapy – Tamoxifen is the first choice for men, but quite a few of the men here were also on aromatase inhibitors, some with gonadotropin-releasing hormone, some not. There is no data on comparative effectiveness of these approaches – an area that needs more investigation for sure.

Dr. Mintzer … I received this from a Facebook contact and thought you might be interested in it.
Bob Gordon
Sent from my iPhone
>
There is a study that shows how tamoxafin extends LE over Aromatase inhibitors in men. I had a discussion with my oncologist and convinced her that aromatase inhibitors were not the same in men
if you want a copy of the study, email me at jtuffield@gmail.com